Rare Disease Spotlight: Living with VCP Disease
Interview By Brandi Fleck

Nathan Peck shares what it's like to live with VCP disease, navigate genetic testing, face progressive disability, and turn uncertainty into action through patient advocacy.
The future is easy to ignore when you assume you'll stay healthy. Nathan Peck doesn't have that option.
Diagnosed with VCP disease, a rare inherited condition that can cause progressive muscle weakness, bone disease, dementia, and ALS-like symptoms, Nathan lives with the knowledge that his independence will likely diminish over time.
But instead of retreating, he has spent the last several years building an organization dedicated to advancing research, supporting patients, and accelerating the search for treatments.
Nathan shares what it actually feels like to live with a progressive genetic disease and why he believes action matters more than fear.
Listen to Nathan Peck’s Interview
Watch Nathan Peck’s Interview
Living With a Rare Genetic Disease
Nathan Peck: My name is Nathan Peck. I am a patient and actually the CEO of Cure VCP Disease. I want to enjoy my independence. I do know what the future looks like. You're thinking every day, "Is this my last day that I'm going to be able to stand up?" Getting out of bed, it messes with you. The patient population was not organized. The scientific community was not really organized. That's somewhere that I needed to channel this fuel. Things are happening.
Brandi Fleck: This episode is Nathan Peck's story.
Nathan is such an engaging and interesting guest. He's a dad, husband, son, and nephew, but also a patient advocate, CEO, and patient of Cure VCP Disease, a nonprofit organization dedicated to organizing the patient population and scientists and bringing them together to make progress on treating and curing VCP disease.
In this episode, we start out with Nathan explaining some of the science behind VCP disease, including mutations of a specific gene, the valosin-containing protein gene, hence the name VCP disease. This disease can manifest in one or a combination of ways, including muscle degradation, early-onset bone disease, frontotemporal dementia, and ALS.
This particular disease is commonly misdiagnosed as limb-girdle muscular dystrophy, myositis, or other myopathies. It's a rare adult-onset disease that definitely runs in the family, so we talk about Nathan's family being researched when he was growing up because of the prevalence of the disease in his family, the ethics of having children, the role of genetic testing, and the importance of getting your financial affairs in order before you get genetic testing.
Then Nathan gets really personal, opening up about what it physically feels like to have VCP disease, the mental toll of having the disease, and channeling those emotions into finding answers.
We talk about what the future looks like for Nathan. It looks like everything from not being able to hold a pizza pan to being mindful of curbs when walking on the street and the importance of human intervention in changing the future. It looks like grappling with losing independence, but it also looks like hope for others after Nathan, perhaps Nathan too.
This episode not only educates you on a rare disease but gives you an inside look at the thoughts, feelings, and efforts of a patient doing his best to advocate for himself and others.
If you or someone you know is struggling with symptoms including, but not limited to, abnormal muscle fatigue, bone pain, or memory issues, this episode is definitely worth a listen.
Of course, this episode is worth a listen anyways because not only is it packed with resources and advice on being your own health advocate, but you'll be inspired by Nathan's passion, drive, energy, and business expertise to start doing whatever it is you've been putting off. You get perspective on tomorrow and the importance of taking opportunities that present in your life.
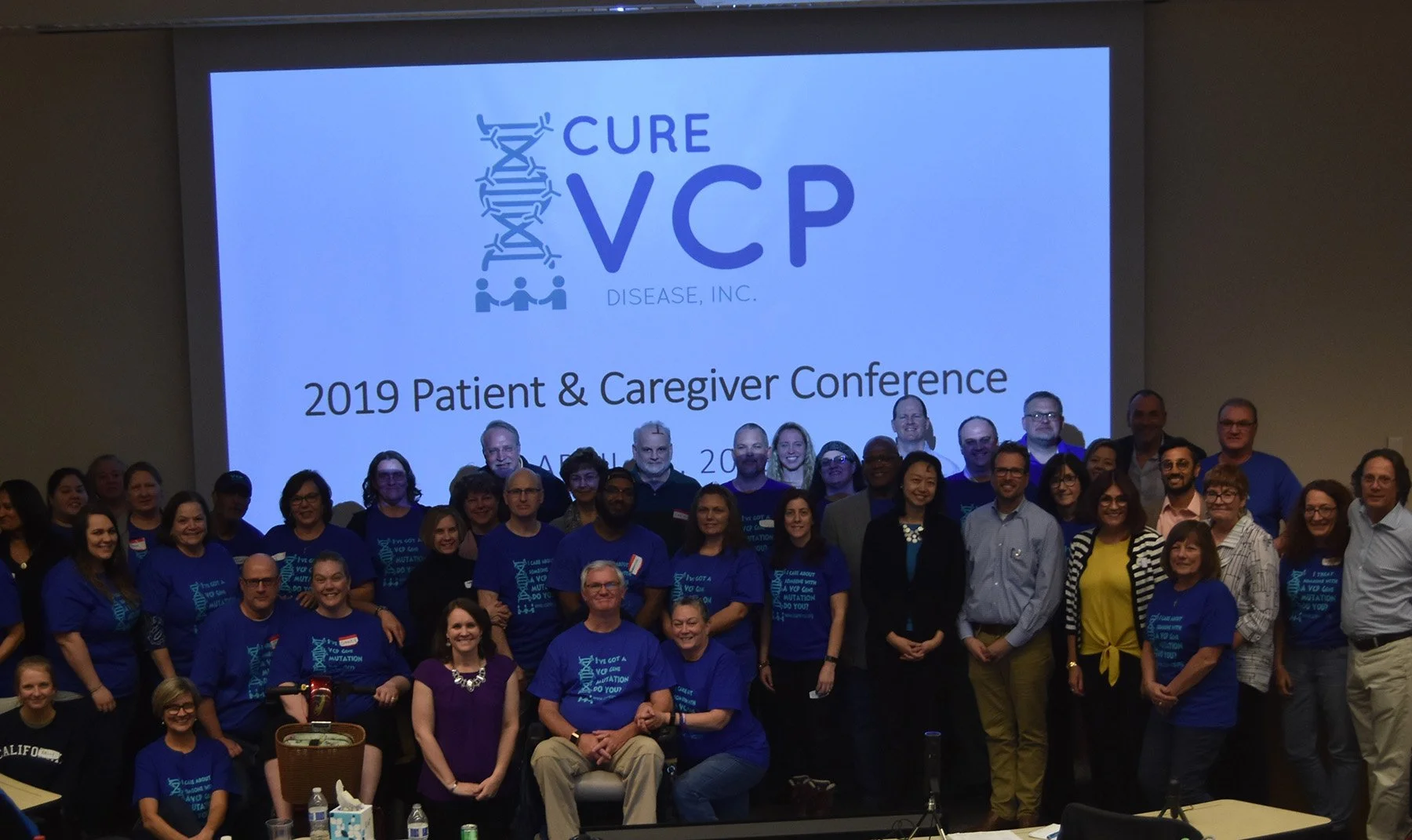
Nathan Peck: My name is Nathan Peck, and I'm 44 years old. I live in South Georgia, and I am a patient and actually the CEO of a patient advocacy organization called Cure VCP Disease.
We started it in 2018. I'm actually a patient with the disease, and my mom is deceased. It's a hereditary genetic disease of the valosin-containing protein, which is the p97 gene. There's a mutation in that gene, and it's what we call autosomal dominant, meaning that if your parent was a carrier, you have a 50% chance of getting that mutated gene.
My mom is deceased from the disease. I have an aunt deceased from the disease, and I have two uncles with the disease.
The symptoms of the disease, there are actually three different what we call phenotypes. I didn't know what that word was until we started the organization.
There's inclusion body myopathy, which is muscle weakness and degradation of muscles. I'm still ambulatory at this time, and that's the phenotype that I have only right now. That's just muscle weakness. I'm still ambulatory. I can walk, but in another couple years I won't be able to.
My mom was unable to feed herself, bathe herself, really do anything. My dad had to do everything for her.
Another phenotype of the disease is early-onset Paget's disease of bone. There are treatments for that, but that's kind of brittle bones, bone pain. My mom actually had that along with the inclusion body myopathy, and I have another uncle that has both as well.
Then frontotemporal dementia is the other main phenotype. There's a lot of discussion about FTD in the news because people are learning a lot more about that disease. It's not necessarily a memory dementia. Your behavior changes significantly. You can't talk.
ALS is also a phenotype, but a much smaller percentage of the patient population.
A patient can get one, two, three, or all four of those phenotypes. That's the disease in a nutshell.
Brandi Fleck: Okay, so VCP disease is valosin-containing protein, and that's basically just the name of the disease?
Nathan Peck: Correct. The valosin-containing protein. There's a lot of research and science going on to try to understand the VCP.
There are actually clinical trials in the oncology, the cancer space, around VCP right now.
It's a basic protein. About 1% of all your proteins in your body are VCP, which I don't know how technical you want to get. Again, I'm no scientist.
It basically unfolds damaged or bad proteins. That's what VCP does. It monitors or facilitates getting rid of them.
Imagine if you were in your house and you never threw away your trash. The trash would just continue to build up and build up. That's essentially what's happening because with the mutated VCP gene, it's not facilitating this process correctly.
The trash just builds up, and bad cells build up. That's what causes a lot of the wasting.
Science still doesn't understand why certain people get certain phenotypes or certain diseases. Why some people get the IBM, some people get the FTD, some people get both. They don't understand why.
Brandi Fleck: Since you did go over a lot of technical stuff there very quickly, is it fair to break it down in layman's terms to say the three main phenotypes are muscle-related, bone-related, and mind-related?
Nathan Peck: That's correct, yeah.
You call them separate phenotypes because it's actually another name for the disease. It's a multisystem proteinopathy because it affects different systems in your body, and they don't know why.
Brandi Fleck: When you say they don't know why, who is "they"?
Nathan Peck: Science. The scientists, researchers, the scientific community.
Brandi Fleck: All right. You said you were a patient. When did you first realize you had VCP disease?
Nathan Peck: I was actually building an arcade system for myself. I had always wanted to build a video game machine, so I was doing a lot of work on the floor putting stuff together.
I noticed that when I would squat on the floor, I had trouble getting back up. I had to give myself a little boost. I thought that was kind of odd because I was very athletic.
When you watch basketball games, you see coaches squat on the floor to get in the defensive position. It was just something that I was having issues with.
I was also doing the P90X workout program because I'd gotten a little bit out of shape. I had such trouble recovering. I literally would get sick when I was trying to recover.
I'm like, "Man, I'm not this out of shape. It's not this bad."
Nathan Peck: I think those were really the first symptoms, or that's the first time I noticed that I was having some problems. I thought, well, either I'm getting old or something's going on.
Because my mom had the disease, I knew there was a chance that I might have it, but you just didn't want to think about those things. At 30-something years old, you're like, man, it's not—I don't know. I don't know.
My mom was still living at the time, and I did not want to go get tested while she was alive. Some other financial reasons too, which I think we might talk about.
Genetic Testing for Rare Diseases
Brandi Fleck: Why didn't you want to get tested while your mom was alive?
Nathan Peck: I didn't want her to have the burden that she passed the disease on to me.
I didn't know at the time, but these things are hard. I think that's why I'm doing what I'm doing today with Cure VCP Disease, because I have three children, and if they end up having it, it's because I was responsible for passing that on to them.
One of my uncles, way back when we started planning for children, was like, "You should not have children. That's irresponsible if you do that."
It was like, "Oh man, buzz off. It's not your business."
But now I understand a little bit more where he's coming from. I certainly feel a big sense of responsibility.
That's why we're doing what we're doing today, because it's all about the next generation. Advocating and creating a cure, a therapeutic, that takes time. It takes a lot of time.
I don't have any misgivings that there's going to be a cure for me in my lifetime, but for my boys, there should be.
Brandi Fleck: Okay. That's an interesting point you brought up that I hadn't thought through before, so thank you for sharing that.
You mentioned the financial reasons why you didn't want to get tested as well. When you say tested, are we referring to genetic testing?
Nathan Peck: Correct. A big topic today is everybody doing 23andMe and things like that, but these are more detailed panels that test for specific gene mutations. Some of the things you see with 23andMe or others are just broad.
This is a specific gene test where, when you're filling out life insurance or disability insurance applications, you have to answer those questions truthfully about what you know.
If you don't know, that's a good thing.
Brandi Fleck: Okay. Definitely want to explore that further because that seems a little difficult to deal with.
But did you actually go through genetic testing at some point?
Nathan Peck: My family had been studied by doctors and researchers, so I think blood was taken from us back in high school before I went to college.
But I never found out the results, and they were de-identified. It was just known within a family, hey, here's what, again, that was science's purpose and their choice of what to do with that data.
But I didn't want to know, and I'm glad I didn't find out at that time.
Yes, we were studied at the time, but it was just a genetic test. I guess they were looking for certain things.
That's how they ended up discovering the VCP mutation. I think 2004 was when that discovery was really made because different families that were studied had similar phenotypes or expressions.
We originally thought this disease was limb-girdle muscular dystrophy, and it's not. It's the VCP mutation. It's kind of a cross between a muscular dystrophy and ALS.
Brandi Fleck: Okay. I would love for you to go a little more in detail about why you wouldn't have wanted to know the results of those tests when you were younger.
Nathan Peck: I think you have to look at and weigh your mentality and how you handle bad news.
It could be that if you didn't have the gene mutation, then it's great news. You can kind of go on, live your life, and it's stress-free.
But if you do have the mutation, even though you might be a strong mindset person or strong mentally, it messes with you.
For example, even when I found out, it wasn't a surprise to me that I had the gene mutation because the symptoms were kind of getting worse. I was feeling some things.
We didn't tell anybody for two years. We told my father. That was it. We kept it quiet, my wife and I. It messes with you. It messes with me now. On the contrary, because I didn't know, I always had a clock in my head. I made some decisions when it came to my professional career.
I always took promotions. They might not have been the right thing to do, or advancement opportunities. I always jumped at those because something in the back of my head was, if I have this disease, I need to generate as much income as quickly as possible.
For instance, I went to MIT for grad school at age 30. I had two children at the time. We sold our house and lived off the equity that we had in our house.
Probably not the wisest financial decision, but it was one of those things that, man, I'll never have another chance. I might not have another chance to do this at this time.
My mindset was always, don't pass up opportunities. Part of that was because of my parents. My parents had big plans for traveling, traveling the world.
My mom had grown up overseas. My dad had never been anywhere overseas, but they had always wanted to travel together.
Once my mom started showing symptoms, right when I was leaving for college, and her condition continued to worsen, those plans were put on hold.
It was really just about survival. I always didn't want to pass up opportunities, and I didn't want to miss anything because I might not have that window.
Brandi Fleck: Sure.
Nathan Peck: I guess my thinking was right. Everybody has a bucket list or things they want to do. I've pretty much done a lot of the things that I wanted to do, so I don't feel any regrets in that regard.
The mindset, everybody's different. Some people need to know. As an advocacy organization, we just try to counsel that, hey, just make sure you have your financial matters in order before you go find out.
But it will mess with you. It does mess with your head.
Again, everybody's different. That's that uniqueness of being human and how people process that information.
Brandi Fleck: Sure. Definitely want to get into the financial aspect of things that you've alluded to since we've started talking.
Real quick though, what did you go to MIT for?
Nathan Peck: At the time, it was called Leaders for Manufacturing, but now it's called the Leaders for Global Operations program at MIT.
It's a dual degree. You get a Master of Engineering in a particular discipline. I did a Master's in Civil and Environmental Engineering, and then you also do a Master of Business Administration, an MBA, from MIT Sloan.
It's a two-year program, about 50 people in the program. It was really focused on global operations and manufacturing. A lot of people in the program had experience in manufacturing.
It was a wonderful program, a wonderful opportunity. Actually, some of those learnings and that preparation have prepared us for Cure VCP Disease.
You know how to approach that because we run, or I run, Cure VCP Disease as a business. It's really kind of entrepreneurial.
Where are the things that we can cobble together to be resourceful when we have limited resources?
From my standpoint, I worked at Dell for eight years and worked in defense. All the different career opportunities have kind of come together for what Cure VCP Disease is.
It's almost amazing how much everything has aligned where it's made it a lot easier. This is just problem solving. That's all it is.
Brandi Fleck: We will definitely talk more about Cure VCP Disease, Inc., but now let's shift into that sort of financial elephant in the room and the problem that people who are coming down with symptoms of VCP disease have to navigate.
What are the financial implications once someone is genetically tested, and what happens once it goes into your medical record?
Nathan Peck: The other piece I forgot to mention is that this disease is an adult-onset disease.
You don't start showing symptoms, according to the research, until your late 30s or early 40s, but everybody's a little different. Some people don't show symptoms until their 50s.
What's different is that in pediatric diseases, genetic testing has to be done to understand what might be going on with your child. Even the parents need to get testing to see if there's something in common.
But for our disease, because it doesn't express until your late 30s or early 40s, everything might be going well and life is good and there's nothing to worry about.
We were blessed in terms of just being thoughtful because we had the information that my mom had a disease that could be hereditary.
Other people don't have that blessing. We've got some patients that were adopted, so they had no inkling that there was this hereditary issue that might happen.
When we talk about it, and certainly it's in the news today, you know, pre-existing conditions and medical insurance.
Right now, you can't be discriminated against because of pre-existing conditions. But that's not true for life insurance, disability insurance, or any other kind of insurance that you might want to get.
You can be discriminated against. When you're applying for these things. And maybe if you're in your early 20s or mid-20s, life insurance or disability insurance is not something you're thinking about. But you
Nathan Peck: If you've had a genetic test done, you need to answer those questions truthfully.

We counsel that we need the data from people that haven't been genetically tested. If you have family members that haven't been genetically tested with VCP disease, we need to know. We need that information.
But at the same time, we have an ethical duty that we try to counsel people that, hey, make sure your life insurance, disability insurance, everything's good and you're comfortable with those levels.
Even after I was diagnosed and it got into my medical record about my condition and disease, I was denied when we tried to increase our life insurance a little bit further. I was denied based on it being in my medical record.
I hope that makes sense. It's just really important to be thoughtful about genetic testing.
Actually, when I had my genetic test done, I went to a Labcorp location, and I can tell the story now. I bribed the Labcorp lady. I paid her 20 bucks just to take my blood because I had a kit to send off to the researcher, but I just needed somebody to draw my blood.
I paid her 20 bucks. She took my blood, put it in the kit, and I sent it off. That way it wasn't in my medical record.
Brandi Fleck: Okay. Yeah, because if you don't have those things taken care of, your affairs in order, and then it goes in your medical record, you could end up not having any means to take care of yourself later.
Nathan Peck: That's right.
I was talking to a patient a month ago. He's now kind of feeling some things. He went to a doctor to talk about his genetics or his family history.
Genetically, that came into his medical record, and now he's trying to apply for insurance and he's having challenges with that because either they weren't going to rate him or offer him insurance, or he's going to have to wait two and a half years where there are no other conditions.
It can't be used in his application, but in two and a half years there's no telling how far he may progress.
He does more of a trade-type activity, which is a little more physical. At this point, that person really can't climb ladders and do other things.
It's a challenge.
That's why we're really trying to educate people. Genetic testing is very important. It's a very important topic, but we just need to be thoughtful about it because I don't think—
I talked at a genetics conference last year, and a lot of geneticists came up to me and said, "Wow, thank you. I didn't even think about that."
Everybody just wants the data, which is super important, but it has real-life ramifications. It has real-life ramifications that could set you back forever.
Again, it's just really important to be thoughtful about it.
Brandi Fleck: Yeah. Does this mean our healthcare system is bad?
Nathan Peck: I'm not even sure it's a reflection of the healthcare system.
I try to put myself in other people's shoes. If I was an insurance company and I knew that this person, if I knew Nathan was going to be disabled or incapable of working the rest of his life, I might not insure him.
I think it's a very prudent business decision.
How would I alleviate that or change that? I don't know. I've actually never really thought about it.
I'm just thankful that we are taken care of because back when I was still healthy and good, I bought a premium long-term disability insurance policy.
One of my uncles was a motivation for this. He had been a teacher and had bought a long-term disability policy. He ended up cashing it in and got kind of a lump sum.
I asked him for years, "Where did you get that? Who do I talk to? What do we do?"
Finally, I was leading a company, and the wealth management people came in. I didn't share too much with them, but I said, "I'm interested in long-term disability."
"Oh, okay. Yeah, we've got that. We can do that."
The benefits of that were that as my income grew, the policy grew. If I changed companies, that policy went with me wherever I went because it was a personal policy. It wasn't a work employment policy.
It also tracked inflation, so as inflation went up, I could increase the income or the benefit on it without having to get a physical.
We paid heavily for it, but now we don't have to worry about anything.
Brandi Fleck: Let's shift. You've talked a little bit about what your adult life has been like career-wise.
Can you give us a little more of a picture into what your life was like before you started exhibiting symptoms in terms of family, just how you lived your life, and things like that?
Muscle Weakness Symptoms in Adults
Nathan Peck: Sure. It was very active. I've always been one of those people who probably worked too much.
I wanted to be the first one in the office and the last one to leave the office. Leadership was very important to me.
Family-wise, I coached my oldest, who's 16 now. I coached all his teams and participated in Cub Scouts as a Cub Scout leader with him.
Just very involved and very engaged. I probably had a problem saying no to stuff. Once I started feeling things, I just couldn't be as active as I wanted.
I was a big basketball player. I loved playing volleyball after work.
But now I can't. My shoulders are so weak I can't get the ball up to the rim.
That's the most hurtful part. My son just had a soccer game yesterday, and man, how awesome it would be to be out there and kick the ball with him.
I need a cane to stand up straight, and if I fall, which I've fallen several times, I'm in a world of hurt.
I still need to be able to be independent. Independence is very important to me.
Being able to travel, for work, I traveled a lot. When I started having more issues, I fell in the airport and was about to get on the plane. My knee was so, oh, it was the worst.
Really, that independence, that's the most fearful thing for me. I'm fiercely independent, and losing my independence sucks. It just sucks.
I'll just be at home a lot because I am retired on disability, and I'll get in the car and just go drive because I want to enjoy my independence while I can.
At some point, having seen my mom and what she went through, having seen what my uncles have gone through, I do know what the future looks like.
I don't like it. Quality of life is really important to me, so that's a challenge.
Brandi Fleck: What does the future look like?
Living With Progressive Muscle Weakness
Nathan Peck: The future is that you continue to lose mobility. Getting off the toilet is a challenge. It's going to be about what accommodations you put in place. Do you get a toilet lift seat? Things that help get you off the toilet.
Certainly using a cane. I have a scooter that I use if I need to walk long distances or go down hills or other things. Going to a conference, I use the scooter.
I've kind of gotten over that. It hurts your pride a lot. The future is, I almost dropped a pizza pan. That thing weighs nothing, but gravity is working against me at this point.
I won't be able to feed myself. It's respiratory failure. That's what you're looking at.
But how fast does that happen? That's what you don't know.
Actually, as an organization, that's what we're trying to measure—what that rate of degradation looks like so that if there were a clinical trial or a drug, you actually know it's working.
You need to understand what that rate of degradation is.
Brandi Fleck: Gotcha. When you fell at the airport, were you able to get back up yourself, or did people help you? How did that go?
Nathan Peck: At that time, I was able to kind of do a push-up and lift myself up. I'd spilled a Coke all over the floor at the Atlanta airport, so that stunk.
But now, if I fall, I would not really be able to push myself up. I need to find a chair or something kind of low where I can shimmy my way up and boost myself up.
Otherwise, if I was somewhere in the middle of a field and I fell, that would not be good. I'd be crawling.
I can still crawl, but a lot of our patients can't even do that. That's how debilitating this is. Your muscles just won't work.
My mom, probably the last two or three years of her life, couldn't even drive her scooter with her thumb or her motorized wheelchair with her thumb.
There are lots of people who are disabled that have those issues, but I think it's hard when you're used to this independence, you had it, and then you're losing it all.
Brandi Fleck: Yeah. What are some of the normal things that people don't think about that you have to think about regularly in terms of mobility or independence or anything like that?
I know you mentioned before this interview about taking flights of stairs or what you have to think about when you're walking toward a curb, things like that.
Nathan Peck: Yeah, curbs. Curbs are brutal.
Curbs are where you could fall down because really the quadriceps are some of the first muscles. Your ankles, quadriceps, shoulders, for most patients, that's what kind of goes.
You really recognize the importance of different muscles in your body.
Stepping up a curb is a lot of quad, and so if I don't have something to grasp or hold on to or kind of push off of, I would not take a curb by myself.
Those handicap ramps that you see are very appealing. They're very useful, and I'm thankful for the Disability Act that kind of mandated that.
But even at my children's school, they have handicapped parking, but it's all curb. There is no ramp. I'd have to go park somewhere else to be able to get into one of the buildings.
We've not made a big stink about it, but it's something that most people don't even recognize or realize.
You can have handicapped parking, but you really need a ramp to get up too because there's a reason. For some of us, stairs. If I can't grab onto something, it's really a lot of arms that I'm using to pull myself up the stairs because my quads are so weak.
Likewise, going downstairs, you're holding on just for dear life to make sure you don't fall and roll down the stairs.
You definitely recognize the importance of certain muscles.
Even now, cabinets, trying to put stuff up in high cabinets. That's the first symptom my mom had, reaching up, and that's becoming more of a challenge now.
With exercise and stretching, those help, but as soon as you stretch, you're just tight again.
Even walking, I definitely focus and concentrate on walking. I walk hyperextended because my muscles are weaker and I don't want to fall.
Even touching things when I'm walking provides stability, versus if you're in a dark room and you can't see where you're going. It can be scary.
Brandi Fleck: Yeah. You said everything feels tight. Are there any other sensations that you get that you did not get before this came on?
Nathan Peck: It's just weakness. It's really weakness.
If anybody's done the Mudder Run or something like that, that's what it feels like for me. It's like I'm just walking through mud. It's hard to move.
You have to be very deliberate in moving. I think the more this goes, I remember my mom talking about the sensation of your arm being asleep. It's like that sensation when your hand's asleep or your arm's asleep and you shake it out.
That's not how I feel now, but it's the slowness and weakness. Literally, I was pulling a pizza on a pan out of the oven, and it was just a certain position that I was in. I almost dropped it because my muscles just gave way.
It really is gravity working against you.
Brandi Fleck: We've talked a lot about the physical changes. Now let's talk a little bit about your mind and your emotions.
When you realized that life was going to change in a big way, how did you deal with that realization, and also how did it impact your spirituality?
Nathan Peck: In the beginning, it's really scary.
We kind of see patients go through different phases. It's probably no different than for a lot of other diseases.
You're thinking every day, "Is this my last day that I'm going to be able to stand up getting out of bed?"
It's really fearful, and maybe a little bit of panic ensues. It's just scary.
When it's harder to get off the toilet, it's like, "Man, am I going to get stuck?"
Then, as you kind of see the sky hasn't fallen and everything hasn't ended suddenly, and it's a slow degradation, you get a little, not peace with it, but you get more comfortable or used to it. You condition into it.
That's where you start to get more comfortable with using assistive devices.
The scooter was like, man, I want to go to Universal Studios with my kids, so I'm going to use this scooter. There are no ifs, ands, or buts. I want to travel. I want to continue to travel.
This scooter is a big thing that enables that. I think in your mind, you just get more comfortable with it.
From my standpoint, certainly there was a lot of anger. I do feel like, look, if somebody's going to get the disease, I'd rather get it than my sister. I'd rather get it than my wife. My wife wouldn't have a predisposition, but I'd rather be the one. I can take the burden.
That anger has certainly been channeled. I'm also a doer, and I believe you've got to do something.
Recognizing that the patient population was not organized and the scientific community was not really organized, that's somewhere that I needed to channel this fuel or this anger.
Brandi Fleck: Yeah.
Nathan Peck: Spirituality-wise, I want to be careful how I say this, but if I fall on the floor, God's not picking me up. He's just not getting me up.
I'm going to have to get up, and I'm going to have to be the one that, whether it's assistive devices or a human being asking for help, does something about it.
In our disease, nothing had been done. There was research going on, but it wasn't until human intervention and people getting together to bring, we have a lot of personalities in our scientific population. Some of them don't get along or don't like each other.
It's our human intervention that is bringing that together. Otherwise, if we didn't do anything, we wouldn't have advanced as much as we have in the past two years.
It's changed my mindset that I've got to do what I can control right now.
I think a lot of people hide behind, "We'll pray for you," or, "We'll pray about this."

Well, that's not going to fix it. Human intervention and people getting on the phone and calling other people, or calling doctors or researchers, that's what's going to move things forward.
I try not to talk too much about it because everybody's different. People's spirituality is what helps motivate them or keep them going, and that's important.
For me, it's not at this point because ultimately I think I know where this is going unless we're able to motivate people, unless there's a breakthrough.
Miracles are supernatural events, and I think we have to be humans that motivate this forward and encourage it and drive it forward.
Brandi Fleck: Sure.
You said that you have channeled a lot of that anger and energy toward finding solutions. Would you say that's why you started Cure VCP Disease?
How Rare Disease Patients Become Advocates
Nathan Peck: Absolutely. My family was studied by the research community. There were certain researchers working on it.
When you have to fill out the same disclosure statement or information about yourself multiple times because it gets lost, that's a little frustrating.
This is the beautiful thing about the internet and the times we're in with genetic testing and advances in science.
You see the patients influencing things. The scientific community says they want it. The FDA says they want it. The NIH says they want it.
They want the patient involved. Nobody's going to look after your disease or address it unless it's you driving that agenda.
A lot of our scientists and researchers are studying lots of different neuromuscular diseases, but my job is to make sure VCP disease, IBMPFD—which is another name for the disease—is number one.
We're not going to let a moment pass by where we're not working on something and staying in front of them.
You know what? They appreciate that. We've spent a lot of time, in the beginning, it wasn't about fundraising for our disease. It was about building credibility.
It was about building trust with these scientists and researchers.
What we really started doing was building a brochure to hand out and articulate the disease, but we also started networking with the scientists and letting them know that we existed.
One of our medical advisory board members, a scientist who I consider a good friend now, we had talked on the phone, but we met him for the first time at an American Neurology Association conference.
It just turned out there was an Atlanta Falcons football game on Monday night, and we invited him to the football game just to get to know him better.
I can't tell you how important that was for the life of our organization because he understands that we're not looking for something from him.
We're here to support. We're here to support all the doctors.
I make that very clear when I talk to these scientists and researchers. I'm not looking for anything from you. How can I help you? How can our organization help you?
The way we're doing that is by identifying patients, organizing our patients, putting on conferences, talking to the FDA, doing those things that make their jobs easier.
Brandi Fleck: Gotcha. Okay. I was definitely going to ask you where you guys started.
How has Cure VCP Disease evolved from those beginning stages to now, and what initiatives do you currently have going?
Nathan Peck: We started because there was the potential of a clinical trial.
One of the researchers had a drug that was being offered to her, and we needed to raise money.
We had a dear friend whose children have a rare disease, and she advised us, "Do not give that money to the academic institution. Do not do it. You need to start a patient advocacy organization."
We were like, "What? What is a patient advocacy organization?" We'd never heard of it.
She's like, "Don't do it. Don't do it."
She was 100% right. We raised that money. Again, it wasn't the researcher. There were a lot of other factors at play, and that's the thing, this is very complex.
We raised a good bit of money for them, and I don't know what's really ever happened to it. It's not important at this point.
What was important was that our friend was absolutely correct. We needed to start an advocacy organization that could help drive some of these activities.
If we wanted to fund research, we could fund research. If we wanted to fund patient support, we could fund patient support.
If we wanted to fund a natural history study, which is what we're working on right now, then that's what we could do.
We could drive the agenda. The first thing was patient identification.
The way we did that was by creating a patient registry where our patients could go in and put in their information. We get asked all the time, "What's the prevalence of this disease?"
We don't know what the prevalence of the disease is because so many people get misdiagnosed or doctors and researchers don't know about the disease.
Creating that patient registry, we did in about five months.
When I would go talk to different companies, drug companies or whoever, they would light up when they heard that there was a patient registry.
That was the most important activity. Then we did a patient conference. A little over a year after we started, we had our first patient conference at Washington University in St. Louis, and we had probably the largest gathering of VCP disease patients in one spot.
It's just these little wins and a lot of listening and understanding, but that credibility is the most important thing.
Nathan Peck: I got a call last week from a scientist asking for our help, to help his research.
It's not us calling him. Now people are coming to us because that credibility has been established.
Brandi Fleck: Okay. What is the natural history study that you mentioned?
Nathan Peck: I was actually on a panel at a Global Genes conference about this.
Natural history study can mean a lot of different things to people, but from our approach, it's understanding the disease in patients across a broad set.
More importantly for us, it's understanding what that rate of degradation of the disease is.
It's collecting biosamples, blood, to be able to analyze that. That's one facet of it. It's looking at people's medical records to understand what commonalities there might be.
It's understanding functionally how people perform. At point A, or time zero, how do you perform? How do you perform at time one? How do you perform at time two?
It's pulling all that information together. It's never been done in our disease. Therefore, if you had a clinical trial or a drug intervention event, how do you know it's working?
You can't just go off of, "Yeah, I feel better." That's one facet of it, but can you actually measure that there's a slowing?
That's the encouraging news in ALS with a particular drug. They slowed the rate of progression of the disease. These are things that we've learned.
If you talked to me two years ago, Brandi, I wouldn't have known any of that. I didn't know what I was talking about. These are things that you just learn in the advocacy space.
Brandi Fleck: Yeah. It sounds like you guys have, like you said, been learning as you go, but methodically working your way through these building blocks.
You keep building on the information you have before to eventually lead to answers. Is that accurate?
Nathan Peck: That's right. We could have taken money and invested in, everybody says, "Oh, you need cell lines and animal models."
We could have done that three or four months in.
The problem was we would have been wasting our money because we've now identified, through networking and talking to researchers and scientists, that they already have a lot of these models. We don't need to reinvent the wheel.
Brandi Fleck: That's right.
Nathan Peck: That's right. Some of that just takes time and understanding.
Trust me, if there's a more impatient person than myself, bring them on. Time is not my friend. Time and gravity are the two forces working against me and our patients.
There are things that you can't do. We've established a scientific focus group.
We were going to conduct the first-ever VCP scientific conference in North America back in September at Caltech, and we had to cancel due to COVID.
What we did instead was create a focus group where we bring 10 to 15, sometimes 20, of the top VCP scientists and researchers together on a monthly phone call.
What we're finding is we started with 10, and now it's ballooning to 18 to 20 because people want to be involved.
We're learning more about the research they're doing, but we're also trying to bring them together.
A lot of them cite each other's work and research, but they've never met in person.
That's unacceptable.We can be a conduit for facilitating and bringing everybody together.
The research probably isn't as important to fund right now. There might be some initiatives, but there's already a lot of money out there studying it. Our role is to bring everybody together and make sure they're talking.
Brandi Fleck: That makes a lot of sense, and it's really awesome what you're doing, by the way, which I'm sure you know.
I do have one more question for you about your study on the rate of degradation.
We talked about this a little bit, but just for our listeners' sake, how far into that are you, and what do you know about that so far?
Nathan Peck: We're trying some different things.
Certainly, COVID has been disruptive. We had some researchers who were going to do a big NIH-funded study. We create centers of excellence across the world where patients can go.
Because things aren't happening, they can't happen. A lot of patients can't travel. The respiratory part of COVID would be terrible for a lot of our patients, myself included.
Traveling and going places is not really an option. The advent of telemedicine and telehealth is a big opportunity for us.
What we've done, we've already started, and actually we had a meeting with the FDA yesterday just to share what we learned. we created a Phase One pilot, a proof of concept.
Using Zoom, and again this doesn't seem like rocket science, but it is innovative, we have our patients get on Zoom and we have a principal investigator from an institution walk them through different activities.
What we did was build kits with all the equipment the person would need.
They don't need to go find quarters or pencils or a dynamometer. We built this thing for them. They have this kit, so everything's standardized. The researcher did everything via Zoom. It took about an hour and a half.
We even bought little step-up platforms because some people are ambulatory and might be able to step up. The researcher can see that, measure it, and score it.
The proof of concept was just to see what issues there might be. We learned some great things through that.
Phase Two is we're going to try to get people to one clinic in the U.S., do the clinical measures, then within a two-to-four-week time period do the same measures remotely.
At six months, do them remotely.
At 12 months, they go back to the clinic and do them again.
I'd love to be able to do it all remotely and not have to worry about going to the clinic, but it is very important to validate that there is statistically no difference between in-clinic and at-home measurements.
Brandi Fleck: That makes sense.
Nathan Peck: That's more the politics of working with the FDA and the scientific community because people are going to try to poke holes in it.
They'll say, "Well, this isn't representative."
Even for the drug companies, if they're doing a clinical trial, they need to feel comfortable with this data.
The learning through this will help us understand how, when that day comes for a clinical trial, we can execute it.
Phase Two will expand to 20 patients. Cure VCP Disease is actually going to fund that work. We're not relying on others for it. Now we have an objective for fundraising to drive those activities.
We're also doing one other thing I'll talk about real quick. We bought 100 dynamometers. That's for hand-grip strength. I went on Alibaba and imported 100 of these dynamometers.
Our goal is to give them to the patient population so that every two weeks they can measure their grip strength.
That might be an indicator of the rate of degradation as grip strength starts to decline.
Again, we're doing that through a Google Form and a Google Sheet, but if we ever want to publish on that data, we need to have an IRB in place.
That's something we're learning about. We're still trying to determine whether we do that through an academic institution or ourselves. There are creative, innovative ways to measure.
Brandi Fleck: What's an IRB?
Nathan Peck: Sorry. That's an Institutional Review Board. It's a third party that reviews a scientific project to make sure it's scientifically valid.
I'm probably butchering the definition a little bit, but if you ever want to publish in a scientific journal, you need to have had an IRB-approved study.
It's a prerequisite.Cure VCP Disease could go run our own study, but if we ever wanted to publish in an academic journal, we wouldn't be able to because we didn't have an IRB-approved study. Ultimately, we really want to publish on it.
Brandi Fleck: Do you have a time frame for when you think you'll have enough data to say what the rate of degradation is?
Nathan Peck: That's a great question. Actually, we don't know. One of our scientists said, "Man, I hope in 12 months we might be able to see a difference."
I can tell you that in 12 months I've degraded, especially because of COVID and being at home more and not being as active.
Certain skills have degraded. Again, how do you quantify that? Our hope would be to begin in 2021 with this remote clinical study.
COVID is going to be a factor because we still have to start people in the clinic. I would hope by the beginning of 2022, or Q1 of 2022, we've answered that question or at least have a better idea.
Certainly our hope is that what we're setting up is all about momentum. We get this study started. If we're able to get more funding for it from other sources, then great.
Otherwise, we'll keep funding it and keep it going. We'll bring on even more patients because that data is going to be important.
Maybe there is endpoint or a biomarker that comes along in that time.
Brandi Fleck: Okay. All right. Well, I'm definitely going to follow you and see how this goes. It's just awesome, the work you're doing.
Nathan Peck: Well, I appreciate that, and I appreciate your support. Again, a lot of this is marketing, educating, and awareness, so this forum is certainly a great way to do that as well.
One other thing, I know we probably need to wrap up, but I learned a valuable lesson talking about publication. One of our researchers, during COVID, had his lab shut down. He didn't know what to do with his postdoc students, a lot of PhD students, and so he said, "Why don't we publish a paper on your patient registry?"
Okay, sounds great. Let's see what comes out of it.
That paper came out at the end of September in the Orphanet Journal of Rare Diseases, and I can't tell you how important it was. It was such a lesson because now I could email scientists or researchers or people who might not know who the Cure VCP folks are and might think, "Get out of here. We don't want to deal with them."
But when we said that we published this paper, we had people coming to us because they said, "Oh, I saw this paper." It gave more credibility to what we're doing and to the disease itself.
That's why, for me, maybe I was the dunce in the room, but actually publishing and having a real publication about our organization and the work that it's doing was really important and extremely valuable.
Lessons From Living With VCP Disease
Brandi Fleck: What advice do you have, just taking all of your life lessons and experience, and what advice or wisdom would you give to others now that you know what you know?
Nathan Peck: I think: no fear. None of us know. I don't know anything about the science of the disease. I know very little. Have we gotten smarter about it? Absolutely. Do we listen well? Yes.
There is no formula for how to do this. Everybody's disease is a little different. Your challenges in terms of the scientific community are different. Your patient population challenges are different.
Really, it's learning from others, what they've done, best practices, little nuggets that you can get from others. But there is no formula for this. There is no prescription.
Everybody has to weave their own journey in terms of how you go about this. You have to be very dynamic in terms of what you do.
Don't be scared of it. Even within our patient population, a lot of people don't understand that we don't know what we're doing, but we're doing something. Things are happening and momentum is being built.
But we weren't scared. I send out newsletters. We do social media. We've taught ourselves how to do all this stuff. Calling on scientists, researchers, bringing them together. I'm not real comfortable doing that because I don't have the academic background for it.
But it doesn't matter. They appreciate it, and things are happening and getting done.
It's really the no fear. If you make a mistake, look, we've got a disease. We're going to suffer as it is. You can't make a big mistake.
One of the big things is paralysis by analysis. You can't analyze forever. To me, inactivity is the bigger sin. Not doing something is worse than making a mistake because that's how you're going to learn.
That's just the same as a professional career. It's no different.
Brandi Fleck: Okay. Well, where can people find Cure VCP Disease and all of your social media? Where can they follow you? Things like that.
Nathan Peck: On Facebook, we're @CureVCPDisease. If you just type Cure VCP Disease in the search bar, you'll find us.
We're on LinkedIn. We have a small presence on LinkedIn. We're on Twitter as well, @CureVCPDisease.
On our webpage, which is www.curevcp.org, you can subscribe to our newsletter. We send out a lot of information within the rare disease space.
We're a Global Genes Foundation Alliance member. You can find us through NORD, the National Organization for Rare Disorders.
Our registry and all the links are on our webpage. We'd love to connect with anybody who is interested in learning more.
Brandi Fleck: Okay. Well, all of those links will be in the show notes, so you guys make sure you go over there, get those, and check it out.
Nathan, thanks so much for coming on the show. It's been an absolute pleasure.
Nathan Peck: Brandi, I appreciate all that you're doing. The pleasure was mine. I appreciate the opportunity.
Join the conversation!
Feel free to share your own experience and let me know if you have any questions in the comments.
Related Posts










Hi, I’m the founder of Human Amplified. I’m Brandi Fleck, a recognized communications and interviewing expert, a writer, an artist, and a private practice, certified trauma-informed life coach and Reiki healer. No matter how you interact with me, I help you tell and change your story so you can feel more like yourself. So welcome!
Find More on the Blog
Topic
- ADHD
- Atlanta
- Black and BIPOC
- DIY
- FAQ
- LGBTQIA plus
- Los Angeles
- Nashville
- Seattle
- St Louis
- St. Louis
- UFOS/UAPs/ETs
- abuse
- accountability
- addiction and recovery
- adoption
- affirmations
- afterlife
- angels
- animals
- anxiety management
- art
- astrology
- atlanta
- awakening
- beauty
- behind the scenes
- being human
- body image
- body work
- boundaries
- brandi fleck
- breathwork
- bullying
- burn out
- burnout
- cancer
- career
- caretaking
- chakras
- channeled
- clarity-dive
- clarity-practice
- clarity-primer
- clean products
- coach
- codependency
- communication
- community
- confidence
Recent Blog Posts


Visit the Full Podcast Audio Archive

Affiliate
